Last March, the coalition government’s Health and Social Care Act passed through parliament. It represented a radical shake-up of the NHS and has brought extensive changes to the entire NHS and public health landscape, setting out a major programme of reforms to restructure healthcare services and public health responsibilities.
A new public health structure, born out of these wide-ranging reforms, came into force on 1 April 2013.
Background
The coalition government’s strategy for public health was originally laid out in the white paper Healthy Lives, Healthy People, which envisaged moving to a more local and patient-focused health system. The White Paper proposed changes to the way public health services are commissioned and delivered, which were subsequently formalised in the Health and Social Care Act 2012.
The rationale for the change is to better meet the needs of local populations, and to enable the integration of public health into local systems and services, acknowledging the importance of local issues and the social determinants of health (eg housing, education, financial security and the built environment).
The changes are also driven by a need for the NHS to find £20bn of efficiency savings by the end of 2013/2014, as well as ongoing cost efficiency opportunities within a national health system that’s pressured by rising levels of chronic conditions and an ageing population with complex social care needs.
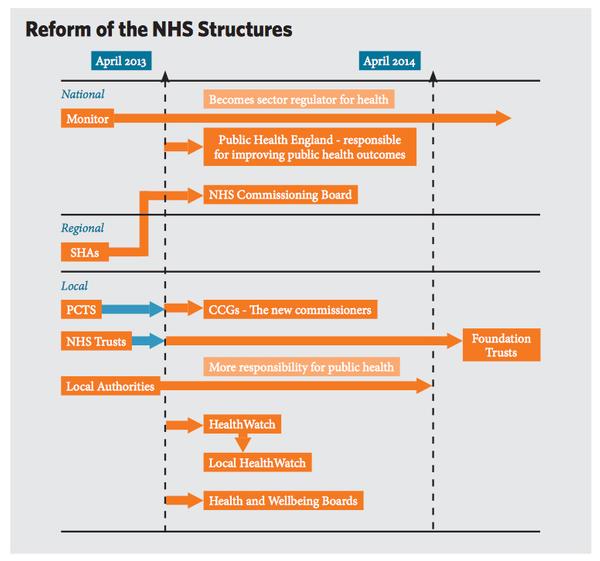
All change
The key changes that came into place on 1 April 2013 include:
• Primary Care Trusts (PCTs) are replaced by Clinical Commissioning Groups (CCGs), giving greater control to GPs in the commissioning of primary, secondary and social care.
• Local authorities will now be responsible for all areas of public health, including tobacco control, locally-led nutrition initiatives, public mental health services, increasing levels of physical activity in local populations and decreasing inactivity, managing chronic conditions and obesity levels, and initiatives on workplace health. Local authorities will be guided by a new structure, Public Health England, on how to distribute their £2.7bn ringfenced public health budget.
• Local authorities will need to demonstrate improvements in public health outcomes, measured in terms of progress against indicators of local health needs. These needs will be set out by the local authorities and CCGs in Joint Strategic Needs Assessment (JSNA) and reflected in Joint Health and Wellbeing Strategies (JHWS).
• GPs are charged with making decisions on commissioning – prescriptions will come out of their own budget, so they will be seeking cost-effective solutions and preventative interventions.
The reforms mark the first time there has been structural recognition of the importance of prevention in healthcare and the role of public health. Physical activity levels among the UK population are one of the indicators in the Public Health Outcomes Framework (see below) – that will be used to measure the outcomes of the changes detailed above.
Measuring outcomes
The outcomes of these changes to public health delivery will be measured through a number of frameworks:
NHS Outcomes Framework
A framework to provide a national overview of how well the NHS is performing, wherever possible in an international context. It will also act as a catalyst for driving quality improvement and outcome measurement in the NHS by encouraging a change in culture and behaviour, including a stronger focus on tackling health inequalities.
Quality Outcomes Framework (QOF)
A voluntary annual reward and incentive programme for all GP surgeries in England, detailing practice achievement results. It’s not about performance management but rather resourcing and then rewarding good practice.
Public Health Outcomes Framework
From April 2013, all local councils will receive a ringfenced budget (a share of around £5.2bn based on 2012/2013 funding) for public health spending, and will be able to choose how they spend it according to the needs of their population. There are 353 councils in England and their performance will be measured against this framework, of which physical activity is one of the sixty-six indicators.
Other indicators include: sickness absence rate, excess weight in four- to five-year-olds and 10- to 11-year-olds, excess weight in adults, recorded diabetes, falls and fall injuries in the over-65s, mortality from causes considered preventable, mortality from all cardiovascular diseases, mortality from cancer, and health-related quality of life for older people.
So what’s the situation now?
As of 1 April 2013:
• The NHS Commissioning Board has taken on its full statutory functions as the national independent body to allocate resources to CCGs and provide commissioning guidance for predominantly primary care services.
• Public Health England is established as an executive agency of the Department of Health and will allocate ringfenced budgets (weighted for inequalities) to local authorities to commission public health services, build evidence bases and co-ordinate service integration.
• Clinical Commissioning Groups are established and assume statutory responsibilities for the healthcare budgets of their local communities (211 in total). GP practices must be members of either an authorised CCG or shadow CCG.
• All Strategic Health Authorities and Primary Care Trusts are abolished.
• Health and Wellbeing Boards are established and assume statutory responsibilities (see p24).
• Local authorities have taken on new responsibility to improve the health of their populations. They will have employed directors of public health, received ringfenced funding for public health, and started the process of developing their local JSNAs and JHWSs through the new HWBs.
• Local HealthWatch is established to give local people a say in how health and social care services are provided.
• Monitor takes on the role of economic regulator for all providers of health and adult social care services, with all providers of NHS services expected to hold a Monitor license.
• Health Education England takes over strategic health authorities’ (which previously oversaw local NHS trusts) responsibilities for the areas of local education and training.